One of the few things that everyone can agree on for PDS is the sex ratio. The general consensus (dangerous term to use!) is that many more men than women have PDS. Figures from reliable sources (dangerous term to use!) are between 3:1 to 5:1.
I also looked at the sex ratio during my statistical analysis of the
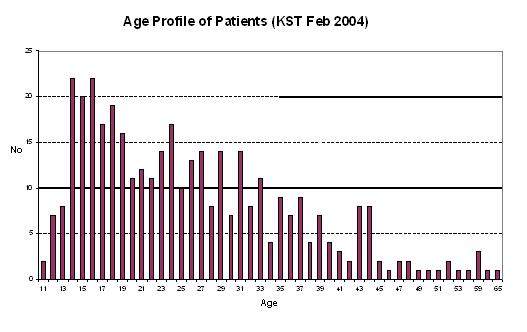
Kassel Stuttering Therapy (KST) sample. It is always a good idea to make up your mind on your expectations BEFORE looking at the actual data. The human mind is such a skillfull master in twisting your interpretation of the data to make it fit its preceived worldview. So what should I expect? Well, the KST sample is a subset of the PDS population (i.e. all members in the KST sample are members of the PDS population). So it is interesting to see whether the sample is a representative snapshot, i.e. similar to the PDS population, or whether the KST fluency shaping therapy only attracts a certain type e.g. attracts more men than women.
The KST sample could be biased, because 1) women are more likely to seek therapy than men, or the opposite. 2) women are turned off by fluency shaping therapies as they mostly involve speech exercises, or the use of a computer, but have limited focus on pyschological/social issues. OR, the two effects could also balance out, i.e. the women might be more eager to attend therapy in general but less likely to go to fluency shaping therapies.
Intuitively (dangerous term to use!), the two effects are probably not very significant. For effect 1), women might be more likely to seek help in general, but I think, due to the clear and apparent handicap of stuttering, men will also seek help or might be pushed by others to do so. For effect 2), most people with PDS are rarely well-informed on different choices or able to make different choices of equal costs to them. Often, they/we are "desperate" for help and would to do pretty much everything.
The KST sample contains 385 patients. And the split is 305 men and 78 women. Two of them had no sex (entry in the database). This gives a ratio of 1:3.9, so roughly one man to four women. Thus this is pretty much in line with the general consensus. Unfortunately, it does not allow me to exclude effect 1) or 2). I could exclude effect 2) if I could compare the sex ratio to other therapy forms. I could exclude effect 1) if I had very reliable data on sex ratio, something like large scale studies with a number like 1:3.34 plus error estimates. Unfortunately, I dont have free access to academic literature to dig out numbers. And secondly, I guess that the numbers are not very reliable anyway, so it's not worth the effort. (Is this an example of my mind twisting my thinking to accommodate my laziness?? :-) So for the time being, I will conclude that there is no clear difference in gender between people attending the KST fluency shaping therapy and the general population.
A side issue is whether the sex ratio is constant across culture. To my knowledge, there is no difference at all. But, I found this citation: "In Canada, the United States, most European countries, and Japan, people who stutter make up about 1% of the population. In the West Indies, 3-4% of the population stutters. African countries seem to have the highest prevalence of stuttering with about 8-9% of the population stuttering." (
Source ) I refuse to believe this. My guess is that the difference comes from different definitions, and bad statistics. Unless it is a genetic effect. You are welcome to disprove me. Also, if it were true, then you would expect differences in sex ratio, as gender effects differ across different cultures, or not?
I did even more Internet searches on sex ratio, which has inspired my next post's title "How myths are propagated".